Tumors lymph nodes
The lymph nodes may develop primary and secondary (metastatic) tumor.
The most numerous among the primary neoplasm of lymphoid tissue is a group of regional tumors, originating from malignant lymphoid and, apparently, hystyotsytarnoho rostkov. It malignant lymphoma. These include:
- Limfogranulematoz;
- Lymphosarcoma;
- Retikulosarkoma;
- Multiple myeloma (myeloma).
Clinically, these a manifest increase in tumor lymph node or group of nodes any one, least two areas of the body. Lymph nodes are painless, varying density, moving, not soldered or welded together. Changes in the blood is not observed. Later as the disease progresses sequentially affects the lymph nodes to other areas of the body, spleen, liver, bone marrow, etc..
Nodular lymphosarcoma
Nodular lymphosarcoma (follicular lymphosarcoma, gigantofollikulyarnaya lymphoma, makrofolliku- lyarnaya lymphoma, germinoblastoma, tsentrotsytoma, tsentroblastoma, Brill's disease, and other Simmersa.).
The tissue specimens found significantly enlarged lymph follicles, consisting of prolymphocytes or limfoblastvv, surrounded by small lymphoid cells. The disease is characterized by slow progression. With the development of the pathological process the boundaries between large cells (follikulami) and their surrounding small lymphocytes become less clear.
In cytological preparations punctate of lymph nodes are found prolymphocytes or a mixture prolymphocytes with lymphoblasts, rarely observed lymphoblastic and immunoblastic forms. Identified cells in mitosis. In cases, when punctate obtained not from the tumor area, lymphocytes predominate in the formulations.
Lymphosarcoma with nodular growth must be distinguished from reactive follicular hyperplasia lymph node, which is characterized by the presence of numerous mitotic figures and marked macrophage reaction. When reactive hyperplasia may be present in the formulation components of chronic inflammation. It plays a role and the patient's age. Reactive hyperplasia of lymph node in children and young people. Nodular lymphosarcoma occurs in children is extremely rare, and adolescence is not found.
Diffuse lymphosarcoma
There are six morphological variants of diffuse lymphosarcoma.
Limfocitarnaâ lymphosarcoma (well-differentiated lymphocytic lymphosarcoma, zlokachestvennaya lymphoma, lymphocytoma)
Microscopic examination revealed a punctate lymph node cells, morphologically similar to mature lymphocytes; sometimes marked nuclear polymorphism. No mitotic figures.
Cytological and histological even differentiate this tumor with chronic lymphocytic leukemia on the basis of cytological and histological examination even without clinical data, pictures of the blood and bone marrow is not possible. When leukemization process, t. it is. lymphosarcoma progression with infiltration of bone marrow and peripheral blood, the general picture of the blood and bone marrow, similar to those of chronic lymphocytic leukemia.
Limfoplazmocitarnaâ lymphosarcoma (limfoplazmotsitoidnaya zlokachestvennaya lymphoma, limfoplazmotsitoidnaya immunotsitoma)
The punctate tumor lymph node cells are found, prolymphocytes and plasma cells in various combinations. Among the tumor cells can be detected typical plasma cells and plazmatizirovannye, t. it is. cell types of mature lymphocytes or prolymphocytes, but with a wider basophilic cytoplasm.
Sometimes the number of plasma cells plazmoblastami presented with symptoms of atypia and even immunoblast. Among the lymphoid cells except lymphocytes and prolymphocytes sometimes there are lymphoblasts. Such a combination of cellular elements can occur in chronic lymphocytic leukemia, Waldenstrom's macroglobulinemia, and heavy chain disease.
When painting on glycosaminoglycans (mukopolisaxaridы) cytoplasmic (or nuclei) tumor cells detected PAS-positive globular inclusions, resistant diastasis. Expected, it immunoglobulin M, cuts G or A, which are produced by cells lymphoplasmacytic lymphosarcoma. In the blood plasma can see the contents corresponding immunoglobulins, what, apparently, due to the violation of the mechanism of secretion.
Lymphoplasmacytic lymphosarcoma can be transformed into immunoblastic lymphosarcoma.
Prolimfocitarnaâ lymphosarcoma
The punctate tumor cell type found prolymphocytes, among which there are isolated lymphoblasts.
The substrate prolymphocytic lymphosarcoma may also be cells of germinal centers of follicles, small or medium-sized with nuclei, having a characteristic recess, fine chromatin and scant cytoplasm blednookrashennuyu. Such nuclei are called split.
Prolymphocytic lymphosarcoma cleaved (germinocitoma, tsentrotsytoma, malignant lymphoma cells of the germinal centers of the follicles) characterized predominantly nodular growth.
A version is also prolymphocytic lymphosarcoma sclerosing lymphosarcoma, at which the growth of fibrous connective tissue in the form of strands. Cellular composition may be lean punctate. This type of lymphosarcoma often localized in the groin and parietal (parietal) lymph nodes, while in the nodular form of Hodgkin's disease, which is sometimes necessary to differentiate the disease, It affects mainly the cervical and mediastinal lymph nodes.
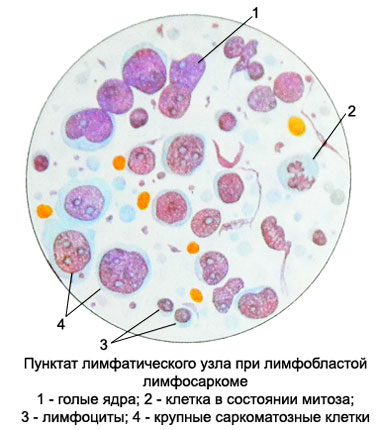
Lymphoblastic lymphosarcoma (poorly differentiated lymphosarcoma, zlokachestvennaya lymphoma limfoblastnogo type, tsentroblasticheskaya zlokachestvennaya lymphoma)
The substrate may be a tumor cell type micro- and makrolimfoblastov. In the first case, they are small, the poor chromatin nuclei, Have one nucleolus, and a narrow rim of basophilic cytoplasm. With the progression of the process of developing acute lymphoblastic leukemia.
Makrolimfoblasty (cells in the 3- 4 times more small lymphocyte) They have a large round or oval nucleus, sometimes irregularly-shaped and jagged-edged with 1- 3 nucleoli, ranging frequently near the inner nuclear membrane. The cytoplasm of the cells is fuzzy contours, basophilic, moderately or blednookrashennaya.
Often there are cells in mitosis.
In some cases substrate tumors are lymphoblasts, having a unique structure of chromatin nuclei, reminding convolutes. This type of tumor occurs in adolescence. Most affected mediastinal lymph nodes. Progressing, the process proceeds to acute leukemia.
Occurs sclerosing variant lymphoblastic sarcoma, wherein the tumor cells are separated by connective tissue cells on. In cytological preparations found lymphoblasts and prolimfoity. The disease occurs favorably.
Immunoblastic lymphosarcoma (immunoblastnaya zlokachestvennaya lymphoma, immunoblastic sarcoma)
Swelling often occurs on the background of immunodeficiency, or immunosuppressive therapy, but can also develop in patients without impairment of the immune system.
The punctate tumors detected immunoblast - Large cells with large round or oval vesicular nuclei, containing one, rarely two large nucleolus, located in the center. The nuclei are located centrally or eccentrically. Cytoplasm abundant, basophilic, intensely colored.

Many cells in mitosis. The suspension of tumor cells give a positive response Koons (na immunoglobulin), Consequently, they are a B-immunoblast. The existence immunoblastic T-cell lymphoma cell nature is not proved.
The substrate immunoblastic cell lymphoma may be plasmocytic cell differentiation. This tumor polymorphonuclear cell. Also immunoblast it occur with atypical plazmoblasty eccentrically located nucleus, and intensely basophilic cytoplasm. There are giant multinucleated cells and histiocytes.
The presence of giant multinucleated cells may require differentiated lymphosarcoma with Hodgkin immunoblastic (Hodgkin's sarcoma). In such cases, repeated puncture biopsy and.
Lymphoma Berkitta (limfosarkoma Berkitta)
It occurs as an endemic disease in Africa and New Guinea. Isolated cases described in other countries. There is the age of 30 years. Lymph nodes are rarely involved. Favourite localization of the tumor - the ovaries, ileum and cecum, thyroid and salivary glands, bones of the face and tubular, tissue of the brain or spinal cord, retroperitoneal adipose tissue.
The punctate tumors detected monomorphic small cell type undifferentiated blasts or mikrolimfoblastov. The kernels round shape, sometimes with small depressions, available from 2 to 5 nucleoli. The cytoplasm is narrow, basophilic, sometimes vacuolated. Many mitotic figures. Often there are macrophages with inclusions of cell debris and whole cells, their presence creates a picture of the so-called "starry sky", that is not specific to Burkitt's lymphoma, as it is observed in other tumors. Leukemization process in this tumor occurs.

Retikulosarkoma
Retikulosarkoma (retikulokletochnaya sarcoma, gistiotsitarnaya lymphoma and others.) - Malignant tumor, develops from cells of the reticular stroma.
The substrate may be a tumor reticular cells and histiocytes, belonging to a system of mononuclear phagocytes. In cytological preparations are found large cells (diameter up 35 m) with large vesicular nuclei of various shapes (rounded, oval, with uneven contours or recess) and one or two nucleoli.
Cytoplasm moderately wide, not always clearly defined, basophilic, painted with different intensity. There are cells with preserved cytoplasmic connections.

There may be the phenomenon of phagocytosis. An important aspect in the diagnostic is to determine the activity of nonspecific esterase; histiocytes in it is high and is not inhibited by sodium fluoride.
Myeloma (extramedullary plasmacytoma, plazmotsitarnaya zlokachestvennaya lymphoma)
The punctate tumor revealed a large number of mature plasma cells. The tumor for a long time may be local, in its generalization bone marrow, usually, no infestation.
Limfogranulematoz – Hodgkin's disease – Chronic malignant lymphomatosis
Limfogranulematoz - Tumor disease of Leukemia Group. Develop at any age (Men suffer 2.5-3 times more often). The main symptom is a swollen lymph nodes, often in any one area.
At the beginning of the disease are determined by single, moving, not soldered to surrounding tissues lymph nodes, in the future they become dense, soldered together and often form conglomerates. The defeat of the mediastinal lymph nodes are often determined by radiographic methods of investigation, used mediastinoscopy with biopsy or diagnostic thoracotomy. For detection of lymph nodes, located below the diaphragm, It can be used diagnostic laparotomy.
During laparotomy performed a biopsy of the lymph nodes available, edge splenectomy and liver biopsy. Histological examination of tissue biopsies to determine the degree of damage of the test and clarify the clinical stage of the disease, it is of paramount importance for the choice of treatment.
As the progression of the process with chlamydia, except lymph nodes, spleen and liver, may be affected practically all organs and tissues: Nervous, bone, lungs, kidneys, gut, endocrine glands, etc..
From Hodgkin extranodal locations is the most common lung disease. According to various researchers, its frequency is from 20 to 45-54 % cases. Often, it is noted and specific pleural. In the pleural fluid revealed lymphoid, reticular cells and Berezovsky-Sternberg.
According to the clinical classification of Hodgkin's disease, depending on the extent of the disease is divided into four steps.
The first stage of Hodgkin's disease
Lymph nodes one area (I) or failure of any organ or tissue (IE).
The second stage of Hodgkin's disease
Lymph nodes of the two or more areas on one side of the diaphragm (II) or the same and localized lesion of any organ or tissue (IIE) on the same side of the diaphragm.
The third stage of Hodgkin's disease
Lymph nodes all areas on both sides of the diaphragm (III), or accompanied by a localized lesion of any organ or tissue (IIIE), or lesion of the spleen (IIIS), or defeat of both (IIIES).
The fourth stage of Hodgkin's disease
Diffuse loss of one or more organs with a lesion or without lymph node involvement.
Localization of lesions in stage IV, histologically proven, denoted by the symbol: L - LIGHT, H - liver, M -kostny brain, O - bone, P - pleura, D - skin, subcutaneous tissue.
Common symptoms of the disease (B):
- Night sweat.
- Body temperature above 38 ° C.
- 3. Weight Loss on 10 % and more for 6 months.
Depending on the presence or absence of one or more common symptoms, t. it is. signs of intoxication, Each stage is divided into two:
- A - in the absence of symptoms;
- D - if present.
Specific changes in the blood picture with chlamydia is not marked. The number of leukocytes may be different. Half of the patients early in the disease observed leukocytosis. Often, especially with involvement of the internal organs, develop leukopenia with relative neutrophilia and shift to the left. Possible and normal white blood cell count.
Neutrophilia is observed regardless of the number of leukocytes and the stage of the disease in 50 % cases. Initially, there may be a stab shift in leukogram, and then appear in the peripheral blood and myelocytes toksogennaya graininess in neutrophilic granulocytes, which increased lipid content, alkaline phosphatase, and a step IV of the process - and peroxidase.
Significant eosinophilia (to 50 % and more) rarely observed (to 3 % cases). In half of the observed decrease in the number of eosinophilic granulocytes, until aneozinofiliya. In the II and III stages of the disease may occur monocytic, which is in the last stage is replaced monocytopenia.
With the progression of the process as a result of toxicity and bone marrow suppression under the influence of cytostatics anemia norm- hyperchromic or character, thrombocytopenia and leykopeniya.
Hodgkin's disease is a characteristic feature increased erythrocyte sedimentation rate (30-40 mm / h, and III and stage IV disease especially - to 70-80 mm / h).
In the study of bone marrow at the beginning of the disease is marked hyperplasia of granular germ hematopoiesis. The number of eosinophilic granulocytes increased, several megakaryocytic cell number unchanged, and the number of red cell number with the growth of intoxication and reduced bone marrow suppression. If it affects the bone marrow punctate tumor in his lymph cells can be detected- granulomas.
Currently, there are different classifications of Hodgkin's disease, trying to link the clinical picture of the disease with morphological changes in the lymph nodes and other organs. Noteworthy morphological classification Lux, Butler and the Hyksos (1966), according to which there are four histological types of Hodgkin's disease.
Lymphohistiocytic version of Hodgkin's disease
Lymphohistiocytic variant is characterized by a predominance of lymphocytes in lymph nodes and histiocytes. When viewing many drugs can be detected isolated small two-bladed Berezovsky-Sternberg cells with a wide light-colored basophilic cytoplasm, as well as single eosinophilic granulocytes and plasma cells.
Nodular sclerosis
When nodular, or nodular, sclerosis lymph node proliferation appear as bands of fibrous tissue. Found Berezovsky-Sternberg cells, their predstadii (Hodgkin's cells) and reticular cells. Berezovsky-Sternberg cells are large sizes, They have a lot of small nuclei or one multiblade core with large nucleoli. Cytoplasmic wide, frothy, light.
Mixed-cell variant of Hodgkin's disease
Mixed-cell variant is characterized by diversity of cellular composition of lymph node. Also lymphocytes, found in preparations of eosinophilic and neutrophilic granulocytes, plasmacytes, reticular cells, Hodgkin cells and typical Sternberg cell Berezovskogo-.

Lymphogranulomatosis with lymphoid depletion
For the option of lymphoid depletion characteristic coarse fiber or a massive expansion of the connective tissue (fibrotic option), the presence of areas of necrosis and a small number of cells of Hodgkin, atypical cells Berezovskogo- Sternberg, a predominance of reticular cells and Berezovsky-Sternberg with moderate sclerosis (reticular option).
Many believe morphology histological variants of the successive stages of development of lymphoid predominance Hodgkin's disease at the beginning of the process until the end of lymphoid depletion of the disease, when the number of lymphocytes decreased significantly.
One of the methods of diagnosis of Hodgkin's disease is a histological and cytological study of drugs. The diagnosis can be considered valid only if it detects a cell preparations Berezovskogo- Sternberg. These cells are multi-specific elements lymphogranuloma. They rounded shape, size from 40 to 80 m, round, bean-shaped nuclei or palmate, is a central or eccentric. In the nuclei of most visible 1-2 very large nucleolus, less fine 5-8. Classic Berezovsky-Sternberg cells dual, wherein the core of the same shape and size, They are like mirror images of each other.
In more mature cells Berezovsky-Sternberg usually have multiple cores. Basophilic cytoplasm, painted in pale bluish or dark blue tone.
Predstadii, or young Berezovsky-Sternberg cells, mononuclear, Smaller. The nuclei of round, centrally located and have two or three large nucleolus light blue, cytoplasm is more intensely colored, basophilic.
When cytochemical study in Berezovsky-Sternberg cells are found glycogen, A nonspecific naftilatsetatesteraza, kislaya phosphatase, RNA-ase and DNA-ase, sukcinatdegidrogeiaza, OVER and OVER-diaphorase, glucose-6-fosfatdegidrogenaza, cytochrome oxidase.
The presence in a punctate lymph node eosinophilic and neutrophilic granulocytes, plasma and reticular cells, lymphocytes, Berezovsky-Sternberg cells, the ratio of which may vary, It creates a mixed picture and allows you to safely put the cytologic diagnosis of Hodgkin's disease. The absence of pathognomonic for Hodgkin's disease cells Berezovsky-Sternberg exclude the diagnosis of the disease, since a similar pattern can be observed in inflammatory and other pathological processes.
Establishing a morphological variant of Hodgkin's disease to determine the approximate forecast. So, when lymphohistiocytic version (the beginning of the pathological process) We can assume a steady flow of disease. In nodular sclerosis possible long duration of the process in the lymph nodes and organs, located above the diaphragm, metastasis to bone. Intoxication symptoms develop later. Mixed-cell variant - the most frequent (in 60 % patients), with an average life expectancy of 3-5 years, It is characterized by more severe than in previous versions. When lymphoid depletion the disease may be rapid and malignant.
The criteria of malignancy include the growth of these indicators, as the ESR, the amount of fibrinogen in the blood, a2-globulin, haptoglobin and ceruloplasmin. Active during the process noted in the cases, If all of these laboratory findings, or at least some of them exceed certain critical values (ESR above 30 mm / h, Fibrinogen ≥ 5 g / l, a2-hlobulynы ≥ 10 g / l, gaptoglobin ≥ 1,5 g / l, tseruloplazmyn ≥ 0,4 Power. ekstiaktsii).
Subject to availability (B) or lack of (A) common symptoms and the presence of (to) or lack of (and) indicators of biological activity there are three groups of patients:
- Aa - with local symptoms (common symptoms are absent, laboratory parameters are normal);
- Bb - a generalization of the process (common symptoms are);
- Ab - with an increase in laboratory values, preceded by the appearance of symptoms of intoxication.
After treatment in patients at Ab indicators of biological activity normalized, in the absence of treatment, these patients go to a group Bb, in which full normalization of laboratory tests after treatment does not occur.